

Hi and Welcome! You may have found this page because you participated in the survey, gave me your email and I’ve emailed you letting you know the results are now ready. If you have come across it some other way, I’m very happy you are here too! If you wish to know the background and motivation for undertaking this project, please keep scrolling down to the part which was published on 11 November 2019.
Photo credit: Gavin Lang.I am very grateful to Gavin for his time and support of this endeavour as well as allowing me to use this awesome photo.
The problem with the results of this survey is that it is very long. What I’ve decided to do is to summarise it first and then the detailed results are posted further down if you have the time and interest in the details.
So what is my conclusionfrom this survey? Despite the numbers being very small, it represents approximately 2% of the current NZ outdoor instructor and mountain guide work force. Obviously the sample is self selected, ie only those interested and invested enough participated. Thank you very much indeed for your kind interest and help!
“if you torture the data long enough, it will confess to anything” quote by Ronald Coase
Summary: I think it is interesting that a fairly large proportion of survey respondents were involved in some first aid management about once a month.
There now exists two rankings for what training topics survey respondents find of highest interest, one all the respondents combined and a separate one for mountain, ski and glacier guides only. They both top with prevention and management of hypothermia , prolonged fieldcare and the mountain guides have those two and avalanche resuscitation as equal top topics.
Some of the topics ( care of the dying patient, stress injury & PFA, performing under pressure and high reliability teams and pain relief ) were not of particularly high interest. These 4 topics are considered of high significance amongst international rescue organisations. I wonder if they were of low interest because they have not traditionally been included in PHEC courses or if they are considered ” too soft and fluffy” or “low kudos”?
No-one was particularly complimentary about Work Safe.
The survey respondents had a pretty high exposure to significant harm events, over 50% in 5 years and for mountain, held & glacier guides this rose to over 70% ( not all incidnets occurred in NZ)
Admitting to sometimes feeling out of one’s dept when dealing with First Aid incidents I believe takes courage and insight.
There are collated results about what time of year, location, duration, cost and format of course most people would prefer. There are also discussions about the need for NZQA qualifications or not, and the willingness of joining a peer training or salaried training provider scheme.
Last but not in any way least, I received several complimentary and encouraging comments on the project, and several expressing their opinions that Outdoor PHEC/First Aid training/ curriculum / qualifications in NZ in its current form is not fit for purpose.
——————————————————-
Results: The first section is about the demographic of the respondents : 43 people responded, 3 were excluded due to not working in the outdoor industry nor being volunteer rescuers. Out of the 40 remaining, 31 work in the outdoor industry. Amongst those 31 professionals there were were 15 ACR ( Alpine Cliff Rescue ( which is either volunteer or professional ) team members, 4 LandSAR volunteers (not ACR) and 14 NZAC instructors: 7 professional, 7 volunteer and one both. 9 of the survey respondents didn’t work in the NZ outdoor industry but 8 of those were volunteer rescuers( 4 ACR and 4 LandSAR) and one was a risk manager. Thus there were a total of 19 ACR and 8 LandSAR respondents.

56% of the respondents job’s fall under the Adventure Activities Operators legislation, thus 44% did not.
28% of the respondents also have a healthcare qualification. There were 4 paramedics, 3 EMTs, 1 St John first responder, 1 NZDF medic, 2 doctors and 1 occupational therapist
42% of respondents were happy for me to share all their answers without de-identifying them. The remainder said they had been frank with their answers because they knew I would respect their anonymity. 70% of the respondents gave me their name and email address in order to be notified of the survey results. I feel privileged and honoured by this trust in me and have ensured that no responses quoted in this analysis can be identified.
35% of the respondents need NZQA unit standards, 65% do not.
This section is about the training the respondents have undertaken most recently and what first aid manuals they own.
| Red Cross PHEC 2.5% |
| St John PHEC 12.5% |
| ProMed PHEC 7.5 % |
| Triple 1 PHEC 17.5% |
| Horizons Unlimited PHEC 17.5% |
| Peak Safety PHEC 0% |
| Wilderness First Responder 12.5% |
| Casualty Care Certificate (Mountain Rescue UK) 2.5% |
| Outdoor Emergency Care (North America) 0% |
| HUNTS by Deer Stalker Association 0 % |
| FENZ responder 5 % |
| Other 22.5%
“the refresher” “I’ve done so many FA courses now it’s beyond a joke” “LandSAR “advanced wilderness 1st aid” “LandSAR PHEC refresh that will not count as PHEC officially, and that I am not sure of the name of, and that has not yet given a certificate…” “Currently WFR, previously multiple PHEC. Former MSC OFA instructor ” “St Johns First Responder, Have done 2 Full PHEC’s incl one at National Ambulance School and 3-4 refreshers” “Haven’t taken a course since Sept 2016” “WFR is a great course. While it is at a similar clinical level to PHEC, the course is longer and involves more hands-on practice of patient assessment and treatment” “Red Cross Refresher (1 day)” “PROMED outdoor refresher, FENZ first aid” ( I have excluded the health care professionals from this section ) |
Is there something which is taught on every first aid course you have ever attended and you’d prefer to be left out of the program? 86% of respondents replied “no”.
Comments included that some courses have poorly planned scenarios. Teaching of interventions which need equipment which is unavailable to the responder ( AED and oxygen mentioned) was mentioned as irrelevant and unnecessary.
First aid manual :44% do not have any first aid manual.Commnets form those who do are found below:
“Jim Duff’s Pocket First Aid and Wilderness Medicine. Particularly for remote overseas trips. I Keep notes from most recent first aid courses. Have ICAR sheets and AvaLife flow chart on H2O proof paper with first aid kit. ”
“Wilderness Medical Associates Field Guide.”
“PHEC Horizons”
“St John CPG, many others i don’t remember the name”
“Cicerone press ” Pocket First Aid and Wilderness Medicine” by Duff and Gormly; and ” Wilderness Medicine” by Forgey.”
“Some outdated ambulance procedures and PHEC field guide (don’t have name to hand sorry).”
“WMA – Wilderness First Aid”
“MSC latest outdoor FA one.”
“NOLS wilderness medicine”
“Horizons course book”
“Wilderness Medicine by Auerbach”
“Remote and Austere Medicine Field guide for practitioners. 2017. Amazing field guide I don’t currently have a copy of. Current edition unattainable. Updating and new edition available early 2020 through CoROM (College of Remote and Offshore Medicine)”
“NOLS/Wilderness Medicine Institute course book (17th Ed 2018) and Horizons Unlimited field notebook”
“Cas Care approx 2014”
“FENZ”
“On average, how many times a year do you use any first aid skills on clients, colleagues or in your free time?” and “If you answered yes to Q6 (LandSAR) ,7 (ARC) or 8 (NZAC volunteer or professional instructor) how often or how many times (over what period)have you used your first aid skills?
I have collated the answers from these questions and drawn a chart of the results. The total is more than 40 due to some dual roles.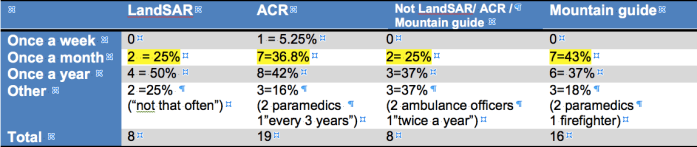
It shows that the population that renders first aid most often is the mountain guides ( including the helicopter ski/ touring & glacier guides). They do so more often than either LandSAR, or ACR or those who are neither of those. The data set is small and the results may not be significant.
How serious are the incidents people have been involved in? I wanted to find this out and phrased the question like this “Have you been involved in the management of a serious harm/ fatal incident since 2015? ”
I initially analysed 3 groups: 1)non LandSAR & non ACR 2) just ACR 3 )All respondents. All the results for those three groups were very similar. Yes 53.8% 21 No 46.15% 18
The only group for which it was significantly different was the mountain, heliski, skitouring and glacier guides. The proportion involved in a serious harm incident rises to 73% ( 11 out of 16 ) 1 skipped the question) Not all of those events occurred in New Zealand.
If you have been involved in the management of serious harm/ fatal incidents or other less, serious incidents, how useful have you found the Work Safe investigators in giving you first aid / medical management feedback? 7 people skipped this question, either because they were developing survey fatigue or maybe for some other reason.
| I have not been involved with any incidents which have been investigated by Work Safe | 65%
22 |
| Work Safe investigators were highly knowledgable and were able to provide valuable feedback | 0 %
0 |
| Work Safe investigators did not appear to pay much attention to this aspect | 15%
5 |
| Work Safe investigators did not seem to be knowledgable with regards to first aid or medical management of patients | 6%
2 |
| Work Safe only engages with higher level management and I am not privy to their discussions | 12%
4 |
I wanted to find out what the “ideal” Mountain Specific First Aid course might look like, so here follows the answers to those questions:
- The preferred time of year to hold a first aid course would be autumn
- and most respondents would like online pre reading combined with a practical course.
- The preferred length is 3 days
- And the preferred cost is $100-500
- 65% or respondents would be happy to become “peer tutors” passing the knowledge on to their colleagues with twice a year in house refreshers using scenarios.
- 35% would be prepared t be salaried instructors on the new course
- 70% prefer scenarios over tutorials, 15% prefer tutorials but 41% think a combination of both is best ,
- 80% like fake blood and moulage
- 66% believe it is useful to have scenarios in the dark
If the new, innovative, mountain specific first aid course (level a bit above PHEC) were not to be a Skills.org or NZQA recognised qualification , you might still have to do a “recognised First Aid course” most likely 29321 “Provide basic emergency care” to tick the boxes, would you still be interested in attending the new course?
73% said yes, 23% said no, 4% commented instead. Below is a representative selection of comments: “Difficult answer.. but l.. Money! I do find up-skilling very important (and have done wilderness first aid courses in Australia in the past because of the inadequate level of PHEC for real life), but there is only so much I can afford to put into my training. The ideal situation would be a course that included workplace required units within it.”
“Why not get it lined up so we do one decent 1st aid course that ticks the box. Save having to pay for two….”
“I would suggest changing title eg to mountain first responder, to reflect the vast difference between first aid/ 6400/3 credits and first responder/ 29321/40 credits”
‘From a H&S view point, It would be a great initiative to be a part of as it will surely provide staff necessary skills above “Provide basic emergency care” that will be utilised on the job daily in the mountain environment. Rather than only a box ticking exercise of having standard 29321 which is more often than not conducted in a classroom and not focusing on industry specific requirements that are special to what we do remotely, especially in the mountain environment.”
“Courses are already very expensive. To maintain my professional status I need to hold a current PHEC or Wilderness First Aid / First Responder certificate. This is a huge cost. I would be interested in doing a high level, NZ mountain specific course because it’s likely I will learn new and useful skills. However to do another basic one where I will probably not learn anything new seems like a waste of money.”
“Could work if considered above phec by NZMGA”
“So long as the course is approved by the police and recognised there would be no need to be unit standards based. Although it may still need some sort of moderation.”
If there were a way in which to obtain clinical, hands on, practical patient care experience (unpaid) would you want to do that to improve your skill?
59% said “yes” 38% said “no” and one person skipped. The comments are below:
“I’ve gained Practical experience through past paid work environments.”
“Probably Volunteer for St Johns but this is time consuming if already working”
“I have done so much training (I counted – I’m now up to approx. 368 hrs first aid specific training), however I see near no trauma on an annual basis. The only way to maintain or advance my skills will to be to work next to experienced practitioners responding to real events. ”
“If time permitted”
“maybe”
“Clinical development is key is keeping skills current and upskilling.”
“But at present work would make that difficult”
“It will be hard to source relevant practical exposure for large number of people.”
“I would if I were working more remotely”
“I’d prefer not to, but in reality if exposure to real experience then it should be part”
There follows some suggested topics, please say if you would want them included in a first aid course(Left side: of minimal interest, right side; of high interest, middle: no strong feelings)
The rankings from highest interest to lowest interest are as follows:
- Hypothemia (76% of respondents said of high interest)
- Prolonged field care
- Shock: How to predict and pre-empt
- Spinal injury: New stuff re. immobilisation and secondary injury
- Chest trauma: New stuff re. flail ( many broken ribs) chest & chest seals
- Traumatic Brain Injury/concussion: New stuff & impact apnea( breathing stops when head hit)
- Pain relief (59% said of high interest)
- Avalanche patient resuscitation / patient care :ICAR/ Avalife2
- Suspension trauma & crevasse rescue
- Bleeding: Packing of wounds, tourniquets & pelvic binders
- Performance under pressure: High reliability teams (52% said of high interest)
- Cardiac arrest: Hypoxic (avalanche/ drowning), high performance CPR (this is what FENZ & St John do now)Traumatic cardiac arrest , AED only if you have one in your kit
- Splinting of fractures
- Care of the dying patient, their rescuers and others on scene (49% said of high interest )
- Anaphylaxis
- Stress injury and Psychological First Aid
- Frostbite
- Altitude (20% said of high interest)
This ranking ( 14 out of 18 ) made me wonder if the 49% of survey respondents who are interested in “the care of the dying patient , their rescuers and others on scene ” might be the same ones who had been involved in one or more a significant harm events?
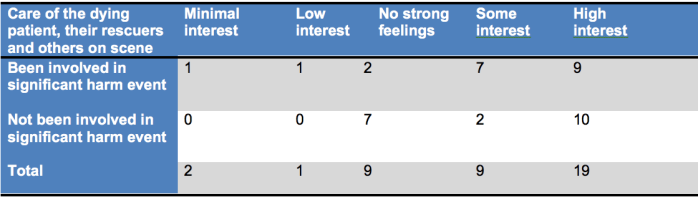
Thus, I think we can conclude it makes no difference, but we have not addressed any historical significant harm events that people might have been involved in.
Stress injury and Psychological first aid was 16 out of 18 in the ranking of topics people wanted to learn about. Only 46% of participants think it would be of high interest. I wondered if there is a difference if they had been involved in a significant harm event.

Once more, there seems to be no predictor in the interest of Stress injury and Psychological First aid whether a person has been involved in a significant war event since 2015 or not. ( As for the “care of the dying patient”, we do not known who has been involved historically.)
The third topic I was surprised about the “luke warm” reception was pain relief.
Only 59% find it of high interest, 33% of some interest and the rest are less interested. I wonder if that is because they do not appreciate the importance of pain relief to the future outcome of the patient ( and the rescuers) as far as PTSD is concerned or if it is based on the fact that they do not have it available to them and don’t believe it is possible to change this status quo? Performance under pressure and high reliability teams was only of high interest to 52% of survey responders. These 4 topics did significantly worse than I had hoped / expected. They are all topics which are considered of high significance amongst professional emergency responders. I wonder if they were of low interest because they have not traditionally been included in PHEC courses or if they are considered ” too soft and fluffy” or “low kudos”?
“I do not believe first aid is useful, since mountain accidents are often instantly fatal.” 85% disagreed, 15% disagreed somewhat. This contradicts the belief by some senior and highly prominent influencers within the NZ outdoor industry that First Aid is of no value. A research project from Wales ” Trauma deaths in Snowdonia: Could more lives be saved?” ( the link is to “scribd”, it is possible to join for a 30 day free trail to read full text) showed that the mountain casualties who were going to die were most likely to do so within one hour of their injury (some instantly, some within the first hour) , which was most often prior to arrival of medical teams with “in-situ” responders ( i.e. mountain guides etc) present on scene rendering first aid. I do not know have the data for the timelines of New Zealand fatal mountain incidents but expect it may be similar. If injuries are not instantly fatal but non survivable, then knowing how to care for that person during the last moments in their life is in my opinion well worth training for. It could potentially help the person who dies, their rescuers and others on scene and also very importantly the loved ones of the dead person.
“I have dealt with first aid situations when I have felt out of my depth and would really like to learn more”
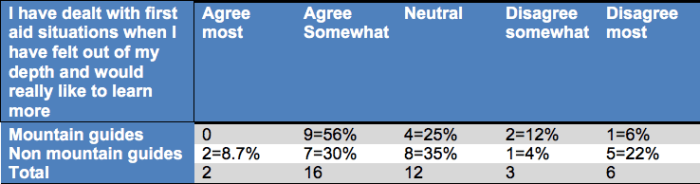
Thus guides either admit to feeling more out of depth than the average person in the survey might mean several things: Their education and training is inadequate They have experienced adverse incidents They have inadequate clinical experience or They are more humble, insightful and appreciate their deficiencies more than the others Dunning Kruger effect
Right at the end of this blog post I discuss what I think contributes towards gaining competence. This is also quite a good blog post on The four stages of competence
This concludes my results of the survey.
Below is the background information and the link to they survey itself. It is still open, if you have not responded but would like to, please do, I will value and incorporate all additional data. Enjoy winter!
Cheers, Malin
——————————
This part below was published 11 November 2019
The green sentence below is the link to my survey, just click on it. It has a branch for professionals and one for recreationalists, you will see the one for you based on your answer to the first question. The survey is estimated to take 10-13 minutes to complete.
Let us create a NZ mountain specific first aid course
Photo credit: Gavin Lang. I am very grateful to Gavin for his time and support of this endeavour as well as allowing me to use this awesome photo.
Disclaimer: This is my personal, individual, independent research project. It is not part of anything I do with Mountain Safety Council or BTRAG or any commercial organisation . It is possible that some of the data which may come from the survey might be of interest to some of those organisations, I hope so, but I ‘m just clarifying that I am not representing anyone else other than myself and I like data. “Without data an opinion is just anecdote” ,” The pleural of anecdote is not data”. I also have no financial or commercial interest in any of this. My only motivator is patient outcomes.
Is there a gap in currently available first aid training which is fit for purpose for NZ mountain/ alpine / snow industry?
I, personally, believe there is. I try really hard to be objective and unbiased but there is not a lot of evidence or data. Or rather, not data which I have found. If anyone reading this has any, please let me know and share it with me. I can be contacted at malinzachau@yahoo.com
How can we find out? How about asking as many as possible of the people who work in the industry? That is what the survey at the top of the page is all about.
Results will be posted here in due course. They will also be discussed as part of the Mountain Medicine Weekend which is being held by the newly formed NZ Society for Mountain Medicine. When: 7 pm Saturday 23 May Where: Aoraki Mt Cook Village Hall. Everybody welcome, RSVP to my email address above. Event postponed until further notice due to COIVD-19 lockdown
Below is an attempt to clarify who the stake holders are with regards to First Aid training in New Zealand , and what their individual purpose is. Apologies for the list being so long, however, I believe that the complexity is part of what I perceive the problem to be. Some organisations currently have minimal involvement but maybe those could be potential future opportunities for promotion of best practice?
Emergency Care training providers: There are many of these in New Zealand, the biggest ones are are St John, Red Cross, Triple 1, ProMed but there are many others, both private and part of education establishments. Some of those have chosen to join the Association of Emergency Care Training Providers AECTP
NZQA: The qualifications authority. Unit standards are developed by industry training organisations and by two NZQA units – National Qualifications Services and Māori Qualifications Services. The Ministry of Education is the only developer of achievement standards, which are derived from the achievement objectives of the New Zealand Curriculum and Te Marautanga o Aotearoa.Collectively, the developers of assessment standards are known as standard-setting bodies (SSBs).
Skills.org :The gazetted standards setting body in the First Aid and Emergency Care domain. They work with industry bodies to ensure that qualifications provide the right skills to employers and industry. They work closely with NZQA, meaning that their qualifications are nationally recognised.
Skills Active Aotearoa is the industry training organisation for the sport, community recreation, exercise, outdoor recreation, dive, snowsport and performing arts industries.
They are a government-funded organisation and our role is promote sport and recreation careers and workforce development, create world-class, nationally-recognised qualifications, and support workplaces to train staff.
New Zealand Outdoor Instructors Association: “NZOIA is an association, of outdoor instructors and guides, which represents and advocates for their interests across a wide range of outdoor disciplines. NZOIA provides credible, accessible and relevant qualifications for outdoor sector professionals. NZOIA ensures and promotes high standards for outdoor instruction to the New Zealand community.” I don’t believe NZOIA deal with any first aid matters but I do know that their annual symposium sometimes has a workshop with some first aid training content. ( I’m hoping to have a chat with one of their team with regards to this. Once I have done so , I will post their comments here)
The old name was NZRecreation Association, now known as Recreation Aotearoa since early 2109 is a charitable body and “represent all professionals in the industry by building capability and networks within the recreation workforce, raising awareness of best practice, and advocating for the benefits of recreation, recreation investment and a highly skilled recreation workforce that meets the needs and expectations of participants.” Their only involvement in anything to do with first aid ( to date ,that I can find) is that they represent the swimming pool sector and recently published a nice little article called “fight or flight in the red zone” basically about performance under pressure as a lifeguard.
New Zealand Mountain Safety Council (MSC): As most of you are probably aware thera has been major changes at MSC in the last few years. The volunteer instructor courses ( some of them Outdoor First Aid) were discontinued mid 2015. This is the current description “The New Zealand Mountain Safety Council (MSC) is a national organisation who has been working for more than 50 years with a mandate to encourage safe participation in land-based outdoor activities. We do this through the development and promotion of safety messaging, by identifying and responding to insights provided by the ongoing collection and analysis of data, and by building partnerships with relevant organisations ” Additionally, the New Zealand Avalanche Advisory (NZAA) is owned and managed by MSC. The NZAA works to support backcountry participants in avalanche risk areas in New Zealand. They do this by providing the avalanche forecasting system in twelve (12) key locations across the country during the relevant avalanche seasons. On their website they have some basic avalanche / mountain first aid advice. This now has a brief and accurate section on hypothermia which I was happy to be involved in updating. One of the avalanche videos mentions patient resuscitation but this content could be improved, hopefully that is work in progress. However, as their role is prevention and safety messaging they advice people to undergo appropriate training and do some signposting for that. MSC also organise the Southern Hemisphere Alpine ( used to be Avalanche) Conference (SHAC) in Christchurch every two years and I may have met some of you there earlier this year.
LandSearch AndRescue (LandSAR) : All their field volunteers have some first aid training and specialist rescue teams like Alpine Cliff Rescue and Avalanche Rescue teams have some additional training, The first aid curriculum for each of these sectors is currently being reviewed.
The New Zealand Mountain Guides Association (NZMGA) is an internationally recognised non-profit Professional Industry Association servicing the standards and competency needs of mountain guides and the tourism operators they work for. The NZMGA regulates the quality of guiding through its training and certification process.On their website they say: “This advanced outdoor first aid qualification is recognised by New Zealand outdoor education and adventure tourism providers” and recommend “Certificate in Outdoor Emergency Care”, see below .The survey has been proofread and shared by NZMGA which I am really pleased about.
NZ Alpine Club : I’ve met with Frances Chrlsworth, Programme Coordinator New Zealand Alpine Club who explained this: The club has recreationalist members of the public and the club engages volunteer instructors and professional instructors. The members decide for themselves if they should have any first aid training and what that should entail. The volunteer instructors policies and procedures, including first aid training requirements can be found here. The recommendation is NZQA 6401 and NZQA 424 and the resin for this is that all the training courses are run within ski field terrain which is being patrolled by ski patrol. The professional instructors are all NZMGA or IFMGA members and thus adhere to the first aid training requirements of those professional bodies.
New Zealand Ski Patrol Association no longer exists. In USA it is responsible for the training of “Outdoor Emergency Care”. This has an extensive curriculum and the fifth revised edition of the book is due out in January 2020. Individual ski patrols have their own arrangements depending on if their ski field also has a doctor attached, and if so, what company that doctor is employed by etc. The level of first aid training required is also determined by the employer.( Commercial ski fields do not come under Adventure Activities legislation because risk is considered low.)
Work Safe Adventure Activities legislation legislate round safety of activities and ensures that the activities are audited. Initially audit bodies were directly recognised by WorkSafe NZ, prior to accreditation by a specialist third party organisation.Adventure Activities legislation and documents
Auditors: There are currently 3 audit providers recognised by Work Safe : Outdoors mark, Adventure mark and Telarc.These audit providers contract auditors to carry out the work.
The New Zealand Resuscitation Council sets the standard for resuscitation in New Zealand. They “foster and promote excellence and consistency in the education and practice of resuscitation”. They publish guidelines which are regularly reviewed. The one for hypothermia is significantly out of date and there is nothing specific about avalanche rescue.
ICAR MedCom is an international panel of experts on mountain emergency medicine, consisting of delegates from the ICAR member organisations. “Our work mainly consists of research into and improvement of mountain emergency medicine in a professional mountain rescue environment. Besides this ICAR MedCom’s task is to set internationally applicable standards for education and training as well as medical guidelines in mountain rescue medicine. This knowledge shall be transfered to our member organisations and into the world of mountain rescue and mountain emergency medicine. The ICAR (International Commission for Alpine Rescue) consists of a medical, an air-rescue, an avalanche and a terrestrial commission as well as a sub-commission for dog handlers.”
————-
Private individual recreationalists in New Zealand are free to chose if they have any first aid training when they are in the mountain environment.
Professionals working in industries not covered by Adventure Activities legislation can simply chose Work Place first aid.
Individuals working in the Adventure Activities are required by work safe to have first aid training “appropriate to the location and the activity” . It is up to the employer (PCB person conducting business) to decide who that might be.
Safework Australia 2018 handles this differently by stating ( page 17 & 18) : “Provide first aid in remote situations
Work Sate NZ refers to the “Primary duty of care” for Persons Conducting Business to ensure their employees and other persons visiting ( e.g. clients of Adventure Activities Operators) are kept as safe “as reasonably practicable”. Employees have a responsibility to take care of each other and should be trained in first aid for this reason.
I was unable to find a NZ version of this but this is from StJohn Victoria Australia (2014) It clearly states that not only does a first aider have a duty of care to their colleagues but also to their clients.
“LEGAL CONSIDERATION :
Duty of Care
A Duty of Care exists wherever there is a relationship between two persons. For example, between partners; between a parent and their child; between the teacher and the student; between the coach and the team player; between the employed First Aider and other employees; between the employer and clients who come into the workplace.
If a person in your care becomes injured or ill, you must do something, within the scope of your training, to assist that person.
A Duty of Care can be breached by either action or inaction (i.e. if you do nothing and the person in your care gets worse). An employer is vicariously liable for its employees’ acts “in the course of employment”.
Historically ( since 2013) the PHEC (Pre Hospital Emergency Care ) course was often chosen by people working in the mountain industry. There have been many revisions of the Unit Standards. A while back the “prepare for transport” and ” manage care whilst awaiting evacuation” were removed from the curriculum. The current 29321 “Provide basic emergency care” replaces PHEC which expires end of December 2019.
There is a slightly different qualification called Certificate in Outdoor Emergency care which is created ,”owned” and delivered by only one training provider in New Zealand, Horizons Unlimited , Christchurch. This is not a ‘Qualification” it is a “training scheme” which also contained the unit standards of “old PHEC” and now the 29321. This training scheme has specific outdoor content. The initial course is 5 days, the refresher is 2 days. If another organisation were to wish to deliver the same training, it would need to do so via a subcontract to Horizons Unlimited. All this information has been given to me via Philippa, Team leader of NZQA Qualifications in Wellington. (Disclosure: between 2013-2017 I collaborated with Horizons Unlimited in a purely voluntary role as medical curriculum advisor. I feel privileged to have Hilary, Jan, Drew and Mike as good friends friends and we still keep in touch. I got the chance to attend some “PHEC refresher” courses in wonderful location with awesome participants. I would mostly chat and listen to accounts of wilderness rescues whilst drinking innumerable cups of tea in-between bouts of paralysis after struggling to walk uphill.)
This similar name should not to be confused with the basic level qualification ( usually done at high school) 424 Assess and manage an emergency care situation during an outdoor recreation activity
The “next level up” qualification form this is the 30 weeks part time course runNZ Certificate in Emergency Care (First Responder) through Whitirea which costs $2700. The course is delivered by ProMed . I am very grateful for the time and help Paul Childs gave me on the phone and here is the information he gave me: The third induction is this Monday 11 November 2019. So fat there have been 10 candidates who have successfully completed the course. Two of those were from the outdoor industry. The course has 60 hours of didactic teaching and 30 hours of self directed learning and 100 hours of operational time. The operational time can be done through St John Ambulance as one option , Wellington Free have not had any vacancies to date. It is up to the candidate to organise the placements themselves and to find a mentor overseeing them. This may undergo some changes in view of paramedic registration and restructuring within St John. The other option is to undertake the 100 operational hours with ProMed at the events they cover as medics, one example being the Coast to Coast race. ProMed has branches all over New Zealand so this offers a good selection of events. The curriculum and training includes the use of drugs like adrenaline and methoxyflurance (full curriculum link above in red) .
If one reads though 29321 it becomes apparent that there is nothing specific in the curriculum about an austere or remote environment where there may be a delay in evacuation and thus possibly the need for prolonged field care (i.e. more than just a couple of hours). The extremely helpful Kharen Hope at the standards setting body Skills org explained that a standards setting body does not write the curriculum, that is up to the training providers.
There are many changes in the pipeline due to “ROVE” Reform in Vocational Education amendment bill in August 2019. The Workforce Development Councils which will be formed will not only be the standards setting bodies, but also the curriculum writing bodies by about 2022, if I have understood correctly what Kharen Hope told me.
I had a long telephone chat with Aidan Tansell, senior advisor Adventure Activities, Work Safe, the day before Skills Active “Outdoor Hui” on 2 November 2019. He has a solid outdoor industry background and a clear understanding of the environments people in the outdoor industry work in. There is going to be a review next year of how the regulations are working and if there are any refinements possible learning from the second round of audits and NZOIA have been discussing this with him.
He explained the rationale behind the very wide statement for first aid requirements as being “appropriate to activity and location” because there is such a varied range of activities and locations and there are diverse first aid qualifications and Work Safe cannot be more prescriptive. He said he knows the good operators train their staff well and that the less good operators might not be doing the same, but the legislation has helped to pull some suboptimal operators up to a better overall standard.
Is there a gap between compliance and competence in mountain specific first aid? (Compliance is about ticking the boxes, competence is about being capable of carrying out the right action and doing so correctly. ) Having undertaken first aid training does not necessarily mean that a person is competent, only regular deployment of clinical skills in the management of real life patients with appropriate oversight and feedback can ensure competence. However, it is more likely that a person who has trained about a medical condition or trauma injury will be competent that somebody who has not undergone any training. This is the reason why the Certificate in Emergency Care (First Responder) incorporates 100 hours operational time. Another way this could possibly have been framed is that a certain number of patient encounters for specific conditions need to be experienced ( e.g. a certain number of unconscious trauma patients and a certain number of patients with for example diabetic hypoglycaemia), but that might be difficult to attain unless one is attached to a busy city ambulance service or indeed hospital emergency department.
—
If you have read this far, congratulations! Your reward is a picture of our lovely Boxer doggo Cassius.

